

Top surgery plays an important role in the transition process and can have significant psychological benefits, in the context of gender dysphoria. Top surgery to address female anatomical breasts entails masculinising the chest through surgical removal of the breast tissue. There are various goals in achieving an appropriately contoured male chest.
These include:
- Removal of the breast mound to ensure a flat chest contour
- Optimal placement of the scar that can mimic the lower border of the pectoralis muscle
- Repositioning of the nipple to a position that is more consistent with a male chest
- Reduction size and shape of the areola
There are two general surgical approaches to ‘top surgery’. This can entail removal of the breast tissue via a double incision (incisions are re-opposed) and reattachment of the nipple as a graft. The alternative method entails removal of the breast tissue via a peri-areola incision (around the nipple).
There are advantages and disadvantages to each top surgery approach and these are outlined in the relevant sections below. The decision to proceed with one or the other can be determined following the consultation process with Dr Reddy in his Sydney & Central Coast clinics and is often determined by your current breast size and how much breast skin currently exists.
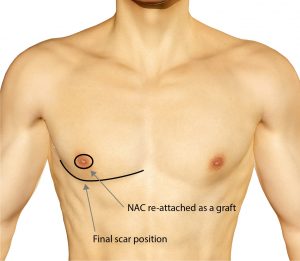
Top Surgery: Approach 1 (Double incision and nipple reattachment)
This is often undertaken to address moderate to large sized breast mounds, as excellent contour can be achieved. It also enables complete freedom in repositioning the nipple. With this approach, pre-operative markings are undertaken based on the location of the planned final scar. The final scar is typically located adjacent to the lower border of the pectoralis muscle. This might not necessarily fall in line with the existing female breast fold. It is important that the new scar is not automatically placed in the existing breast crease, as this may in fact result in a more visible scar.


Following administration of anaesthesia, the new nipple areola size is determined and marked. Both nipple areola complexes (NAC) are removed, and are stored appropriately for later grafting. An incision is made in the pre-operatively determined position, taking into account the above scar considerations. From the upper incision, the breast tissue beneath the skin is removed with cautery. Once the breast tissue below this upper skin flap, the upper skin is re-draped in a downward direction.
The excess skin is then determined and removed. The same approach is taken to remove the breast tissue lying below the lower incision. A drain is typically placed in the space under the skin to enable removal of post-operative tissue fluid. The skin flaps are then sutured together. The nipple is then reattached as a graft. It is important that your surgeon has a good understanding of where ideal nipple position is situated in a male chest. There are certain parameters that are followed in positioning the nipple in the most optimal position. Nipple diameter size is also reduced to ensure a result that is consistent with a male nipple areola complex. Once the position is determined and the nipple areola complex is applied as a graft, the graft is secured in place with a special dressing to optimise graft take. A compression garment is also applied to minimise swelling and support the wound.
- Expert Advice
- Personal Approach
- Highly Respected
SYDNEY & CENTRAL COAST PLASTIC SURGEON

Our Surgery
Information Booklet
Fill out the form below to receive your copy of our surgery information booklet
Top Surgery: Approach 2 (Peri-areolar incision)
This approach is often more suited to a smaller breast as the expected amount of small skin excess can be removed via the peri-areola (around the nipple) incision. Whilst the main advantage of this approach over approach 1, is the avoidance of a scar across the chest, the contour achieved may not be as optimal, as typically a portion of gland is preserved below the nipple to ensure adequate blood supply. This technique is primarily suited to smaller breasts where a significant amount of skin removal is not required.
The technique entails the placement of an two circular incisions (one reflecting the new arola size, and the other larger) around the nipple. The intervening skin is then removed. The breast tissue is then removed through this opening, preserving a small mound to ensure adequate blood supply to the nipple.


This is known as the pedicle. Once removed the skin and breast tissue has been removed, a drain is placed with in the pocket to enable clearance of post-surgical fluid. The outer incision is cinched inward and sutured to the inner incision that surrounds the NAC. The wound is then dressed, and a compression garment is applied. The surgical garment is worn for a duration of 4-6 weeks.

Top Surgery Frequently Asked Questions
WHICH TOP SURGERY APPROACH IS RIGHT FOR ME?
WHAT IS INVOLVED IN THE CONSULTATION?
WHAT DOES THE SURGERY PROCESS INVOLVE?
HOW DO I MANAGE MY SCARS?
WHAT ARE THE POTENTIAL COMPLICATIONS WITH TOP SURGERY?
WHAT IS THE RECOVERY PERIOD?
Top Surgery Before & After



























